

What is equine herpesvirus (EHV)?
EHV stands for equine herpes virus. The two most significant types are Equine Herpes Virus 1 (EHV-1) and Equine Herpes Virus 4 (EHV-4).
Respiratory EHV is endemic in the UK, which means it is everywhere however clinical signs are often mild, and your horse may even have had it in the past without you realising it. The respiratory form of the disease can be caused by both EHV-1 and EHV4: it is reported that 80-90% of horses are infected with EHV before the age of 2 years old.
The neurological form of the disease is rare and obviously is very serious and can be fatal. This form is usually due to EHV-1.
EHV can also be associated with abortion, still birth and severe neonatal illness.
Some horses are life-long carriers, and the virus can be re-activated in these individuals and cause clinical signs and spread to others. Risk factors for re-activation and consequent spread include transport, strenuous exercise, and at equine events.
Most spread of the virus occurs by close horse-to-horse contact, but it can also be spread by sharing equipment such as tack and mucking out tools.
Should you be vaccinating?
The EHV vaccination should not be considered as an alternative to good biosecurity. We strongly encourage horse owners to quarantine all horses newly arrived on their premises.
It is recommended that the following groups of horses should be vaccinated:
· Broodmares should receive their EHV vaccinations every year.
· Racehorses are generally considered high risk and, depending on the jurisdictions to which they are travelling, vaccination may be obligatory.
· Horses which travel away for competitions, particularly when this involves overnight stays in shared stabling.
· Horses which are living on yards where other horses travel away frequently
It is important to remember however that whilst the EHV vaccination reduces shedding of the virus and makes clinical signs milder, it does not necessarily abolish either. However, reducing shedding helps to minimise risk to other horses when a horse is infected with EHV.
There is currently no evidence that vaccination prevents the development of the neurological form of the disease.
To provide effective immunity against respiratory and neurological disease caused by EHV 1 and EHV- 4 a primary course of 2 vaccinations should be given followed by a booster vaccination every 6 months.
- 1st vaccination: Can be given to any horse over the age of 5 months.
- 2nd vaccination: To be given 4-6 weeks after the 1st vaccination.
- 6-month booster: To be given within 6 calendar months of the 2nd vaccination.
To provide effective immunity against abortion caused by EHV 1 and EHV-4 a course of three vaccinations should be given to a mare during her 5th, 7th and 9th months of pregnancy.
To book in your vaccinations please contact Shotter & Byers on 01306 627706.
What is equine herpesvirus (EHV)? Read More »

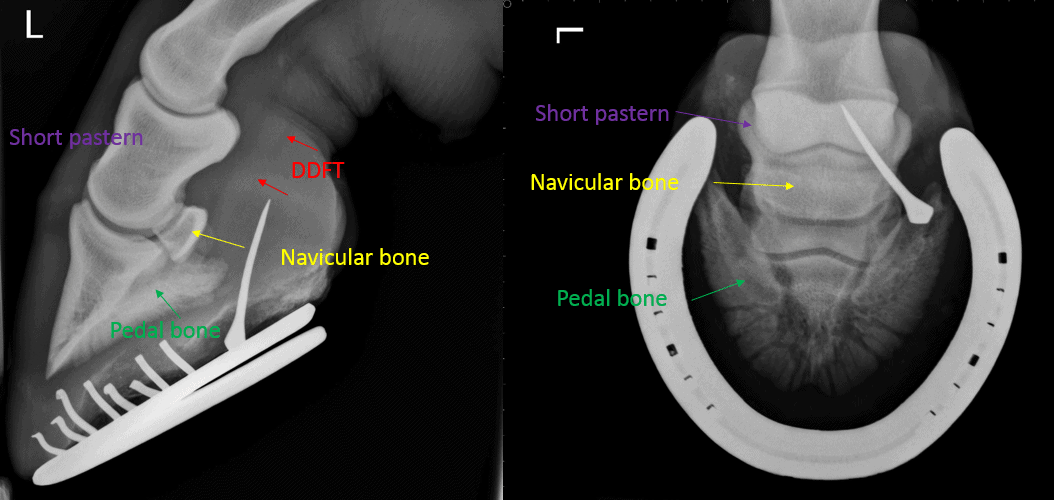 Penetrating wounds of the horse’s hoof are quite common with farrier nails and joinery screws being the most frequent cause. When a sharp object has penetrated the horse’s foot, it can potentially cause damage to the sensitive tissues and structures inside. Depending on the depth and location of entry, the penetration can result in very serious damage, and so a penetrating foot injury should always be carefully assessed by a vet.
Penetrating wounds of the horse’s hoof are quite common with farrier nails and joinery screws being the most frequent cause. When a sharp object has penetrated the horse’s foot, it can potentially cause damage to the sensitive tissues and structures inside. Depending on the depth and location of entry, the penetration can result in very serious damage, and so a penetrating foot injury should always be carefully assessed by a vet.






